The Overlooked Cause of Neck and Shoulder Pain: Understanding the Scalene Muscles
The Overlooked Cause of Neck and Shoulder Pain: Understanding the Scalene Muscles
Author: Jerry Song
The scalene muscles are often overlooked in discussions about neck and shoulder tension, yet they play a crucial role in breathing and upper body movement. When these muscles become tight, strained, or develop trigger points, they can cause significant discomfort, including pain that radiates to the neck, shoulders, and arms.

Anatomy and Function of the Scalene Muscles
The scalene muscles are a group of three paired muscles located on each side of the neck:
- Anterior Scalene
- Middle Scalene
- Posterior Scalene
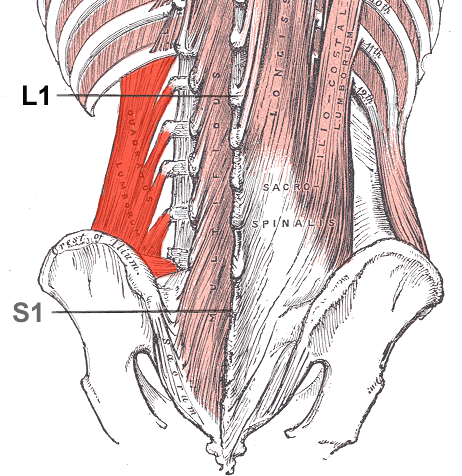
These muscles originate from the transverse processes of the cervical vertebrae (C2–C7) and insert into the first and second ribs.
Primary Functions:
- Breathing: Assist with elevation of the first and second ribs during inhalation.
- Neck Flexion and Lateral Flexion: Help bend the neck forward and to the side.
- Stabilisation: Provide stability to the cervical spine during movement.
The scalenes also form part of the thoracic outlet, where the brachial plexus (nerves supplying the arm) and subclavian artery pass between them. Dysfunction in these muscles can contribute to conditions like thoracic outlet syndrome (TOS).

Trigger Points in the Scalene Muscles
Trigger points in the scalenes can be highly problematic due to their potential to cause referred pain.
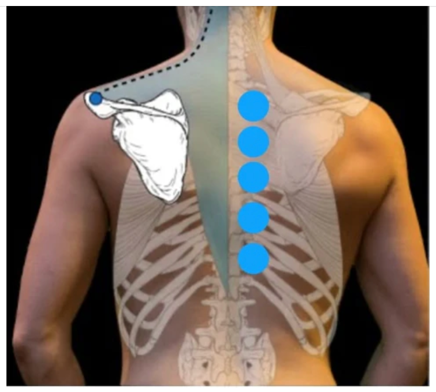
Typical Trigger Point Locations:
- Along the belly of the anterior and middle scalene muscles.
- Near their attachment points on the cervical spine or ribs.
Referred Pain Patterns:
- Pain radiating to the chest, shoulder, and upper arm.
- Numbness or tingling sensations in the hand or fingers, often mistaken for carpal tunnel syndrome.
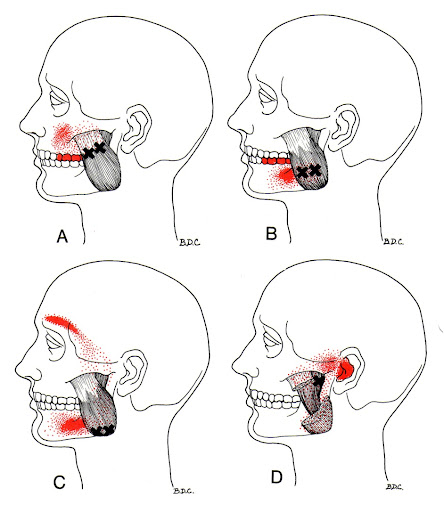
- Tightness mimicking jaw or neck pain.
Trigger points in the scalenes can compress the brachial plexus, leading to neurological symptoms such as weakness or numbness in the arm.
Who Is Susceptible to Scalene Issues?
Certain demographics are more prone to developing scalene muscle dysfunction:
- Office Workers
- Prolonged sitting and poor posture (e.g., forward head posture) strain the neck and shoulders.
- Athletes
- Swimmers, rowers, and tennis players frequently use their upper bodies, leading to overuse of the scalenes.
- Manual Labourers
- Repetitive lifting or carrying heavy loads strains the neck and upper body.
- Individuals with Respiratory Conditions
- Asthma or chronic obstructive pulmonary disease (COPD) forces the scalenes to overwork during breathing.
- Drivers
- Long hours of driving with poor posture or turning the head frequently can overwork the scalenes.
- Stress-Prone Individuals
- Stress often leads to shallow breathing and tension in the neck and shoulders, aggravating the scalenes.
Myotherapy Treatments for Scalene Dysfunction
Myotherapy provides effective solutions for scalene tightness, trigger points, and related symptoms.
- Trigger Point Therapy
- Direct pressure on scalene trigger points helps deactivate them and reduce referred pain.
- Myofascial Release
- Releases tension in the fascia surrounding the scalene muscles, improving mobility and reducing strain.
- Dry Needling
- Targets deep trigger points in the scalenes to release tightness and restore normal function.
- Positional Release Techniques
- Involves gentle movements to relieve muscle tension and improve range of motion.
- Passive Stretching
- Assisted stretches lengthen the scalenes, reducing tightness and improving flexibility.
- Heat Therapy
- Applied to relax the muscles and increase blood flow, aiding recovery.
- Postural Education
- Guidance on maintaining proper alignment to prevent future scalene issues.

Self-Care Tips for Scalene Health
To prevent or manage scalene dysfunction:
- Practice Good Posture: Keep your head aligned with your shoulders and avoid slouching.
- Incorporate Neck Stretches: Perform gentle lateral and forward neck stretches daily.
- Stay Active: Engage in regular exercise to improve overall muscle balance and reduce tension.
- Use Ergonomic Workstations: Ensure your workspace promotes a neutral neck and shoulder position.
- Deep Breathing Exercises: Practice diaphragmatic breathing to reduce reliance on the scalenes during respiration.
- Take Breaks: Avoid prolonged static positions by standing and stretching frequently.
Example case study
A patient (F, 75) presented with a history of neck tightness and stiffness. She goes regularly to Kieser to try and improve her strength and mobility, while also receiving Myotherapy treatments here at Holistic Balance. Upon examination, the patient displayed a more elevated right shoulder than the left due to hyperactive upper trapezius and scalene muscles. She was also limited in her ability to rotate her head to the right compared to the left. After a few Myotherapy sessions that included myofascial release techniques, trigger point therapy, and passive stretching among others, the patient reported an improvement in cervical range of motion, reduced tightness and stiffness, as well decreased soreness in previously sensitive areas. This case highlights the effectiveness of Myotherapy interventions in combination with other modalities, such as physiotherapy or exercise physiology, to manage cervical stiffness and neck tightness. By addressing muscular tension, improving blood flow, and restoring mobility, the treatment provided significant symptom relief and functional improvement. Future sessions will continue to focus on maintaining the progress achieved, with adjustments to the treatment plan as needed based on ongoing assessments.
The scalene muscles play a vital role in neck movement and breathing but are highly susceptible to dysfunction due to overuse, poor posture, and stress. Trigger points and tightness in these muscles can lead to pain, discomfort, and even neurological symptoms. While we’ve focused on the scalenes in this article, it’s also important to note that in most cases, pain arises from multiple contributing factors, including other muscles, joints, and overall movement patterns. For this reason, it’s always best to seek a proper assessment from an experienced therapist to identify the root cause of the issue and develop an effective treatment and self-care plan.
If you or someone you know are dealing with a scalene condition, musculoskeletal pain, or even myofascial trigger points, book an appointment to see Jerry now for an initial consultation so we can assess your condition and come up with an appropriate and tailored treatment plan to manage your pain. Simply click this booking link for the myotherapy initial consultation with our experienced myotherapists.
















































































{kind=link}